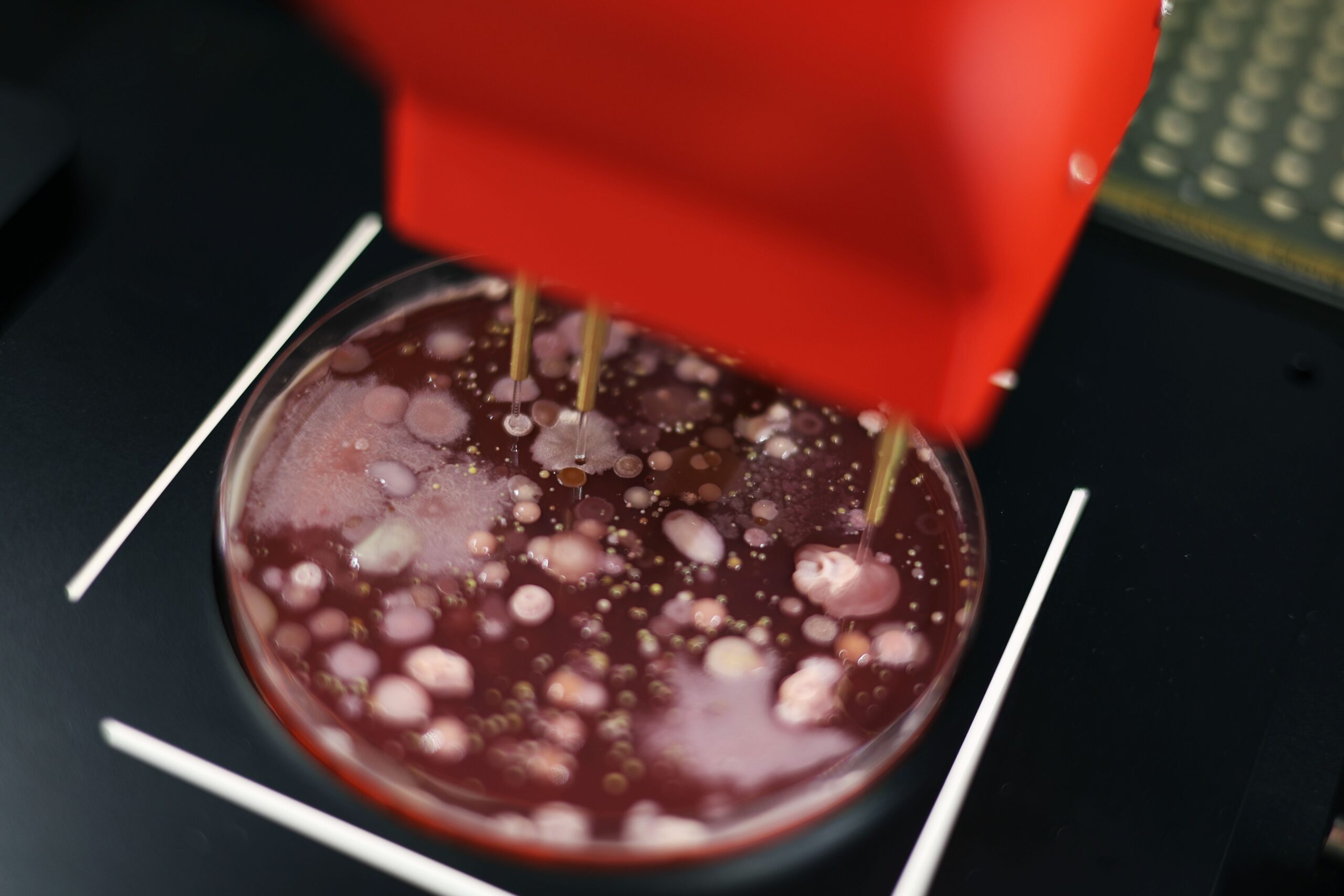
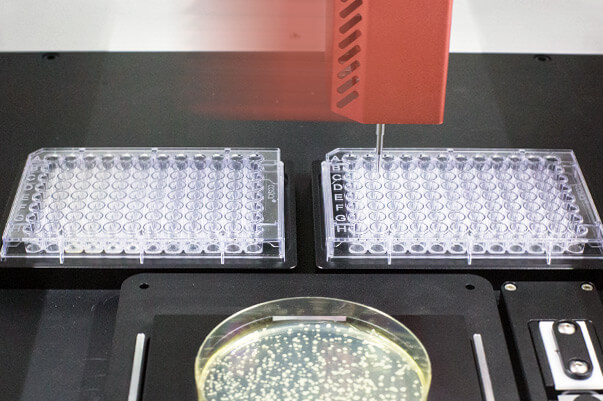
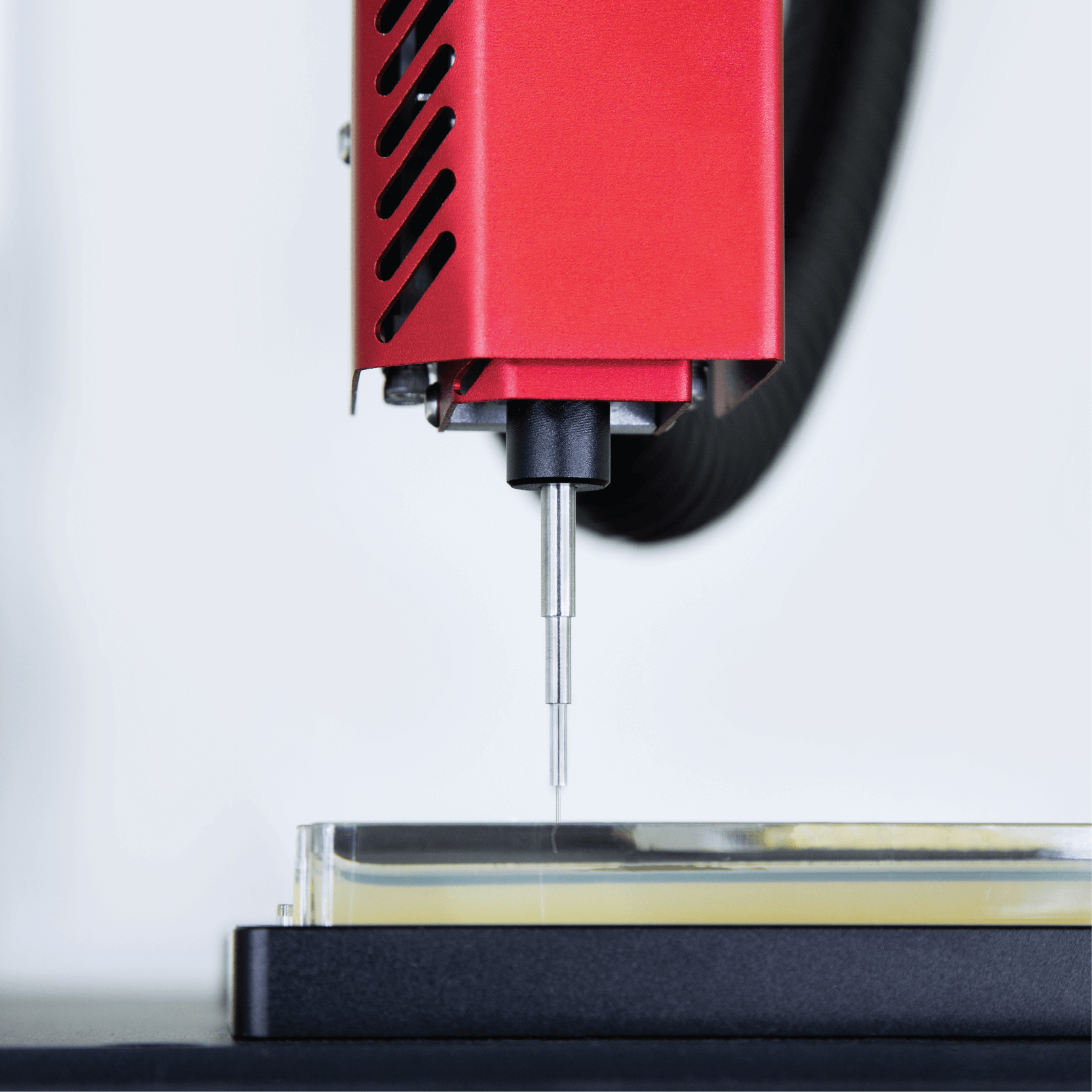
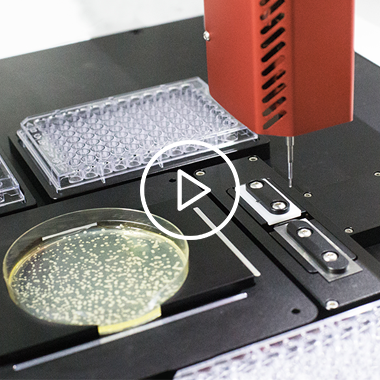
Manually picking colonies is labour-intensive and prone to human error. Eliminate those barriers by automating your workflow with PIXL®.
Exploring Anaerobic Microbiome Research with PIXL Dark
Dr Michal Breker on Chlamydomonas automation
Decoding the uncultivated microbiome with PIXL
Scaling up CRISPR genome editing with PIXL
Your guide to colony picking like a pro
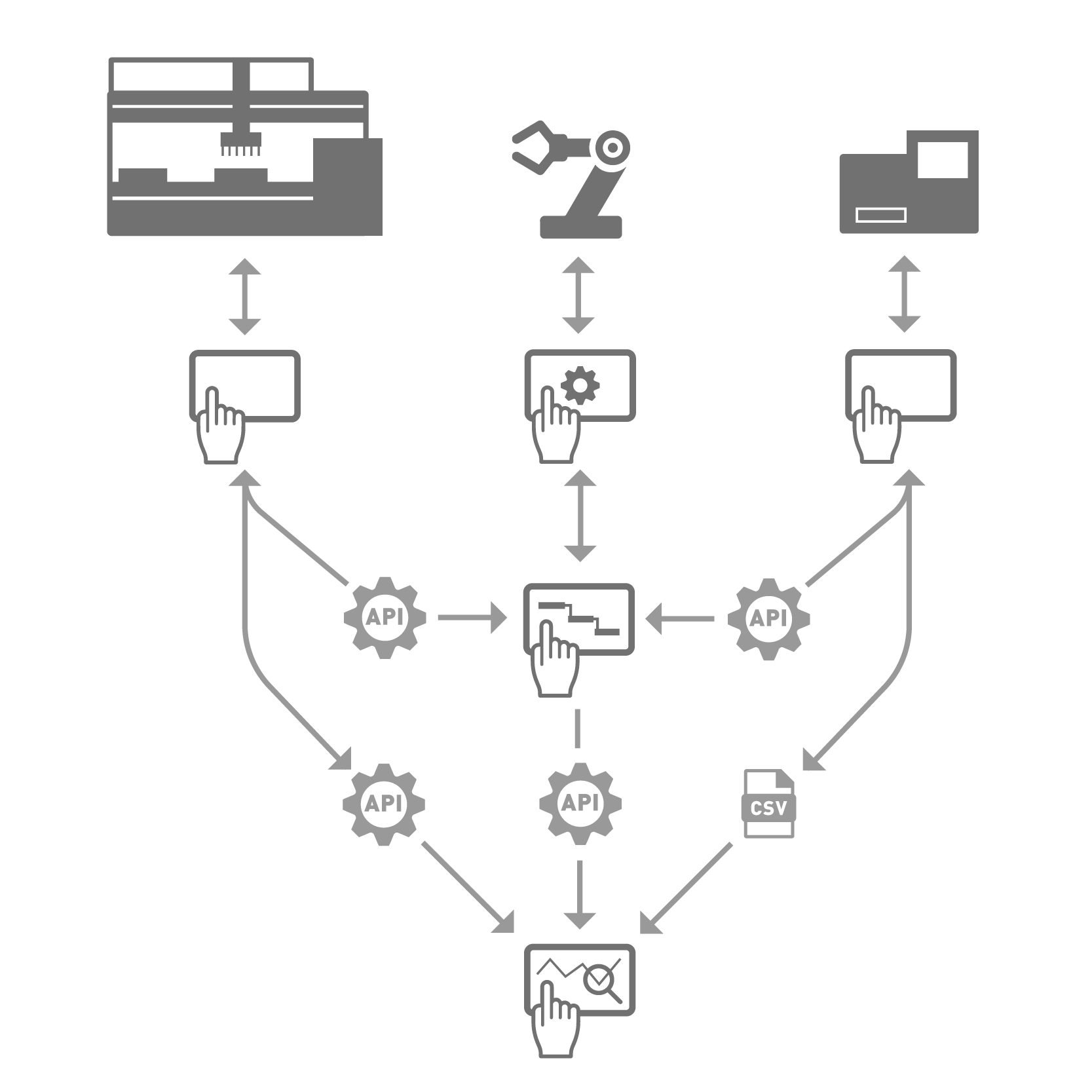
PIXL Command Line Detection
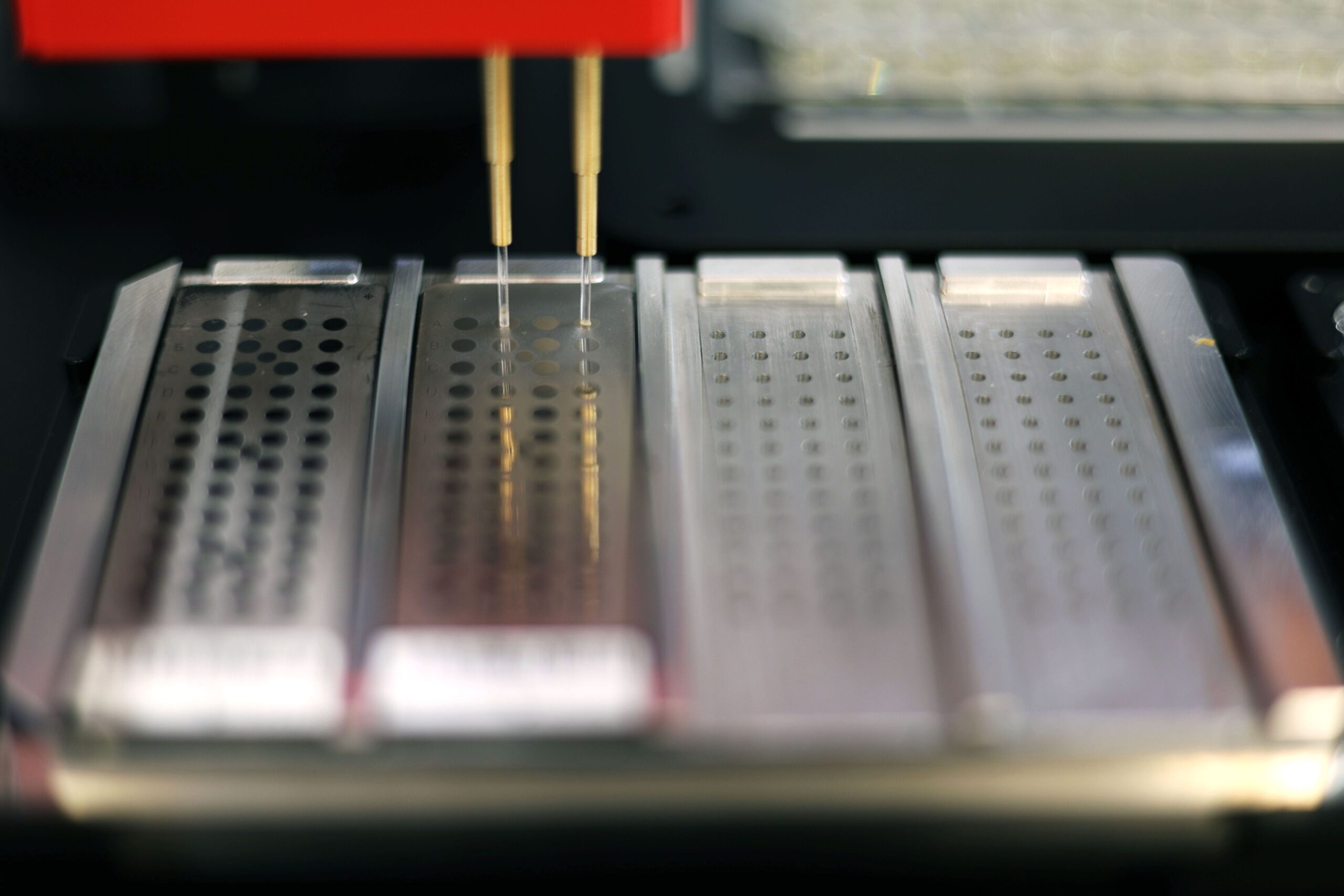
MALDI-TOF mass spectrometry plate prep
On-Demand Webinar | Navigating Microbial Diversity with PIXL Max
On-Demand Webinar | The Dark Matter of the Microbiome
Challenges in Microbiome Research
Harnessing Natural Genetic Variation
AWRI Scales Bioprospecting with PIXL
A benchtop solution for end-to-end automation of MALDI-TOF target plate preparation for bacterial identification
Next generation tools for high throughput genome editing in yeast
From yeast genetics to the secret weapon of bioengineering
Metabolic engineering automated with PIXL Dark
Scaling up synthetic biology – lessons from Singapore
What microorganisms can PIXL pick?
Precision colony picking: Why Reliability Beats Speed
Taking the strain out of strain optimisation
The Synbio Automation Dilemma
Lab Automation: This Checklist Could Save You $100,000s
How to Pick a Picker: What you should consider when automating colony picking
Screening of Scheffersomyces stipitis natural isolates
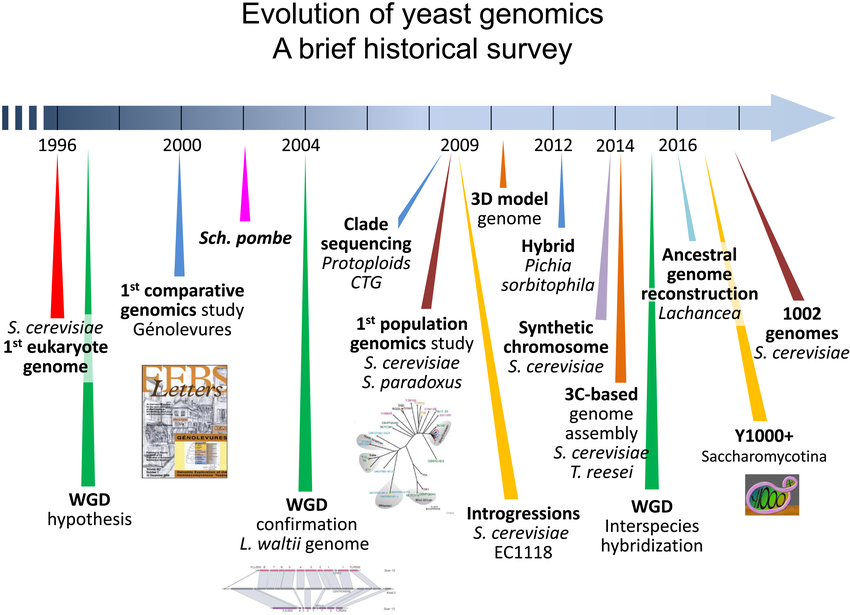
Using yeast to untangle the complexity of life
Considerations When Buying a Colony Picker
Automating MALDI-TOF sample preparation protocols to facilitate bacterial identification.
The benefits of automating colony picking
Lactobacillus in probiotics and food production
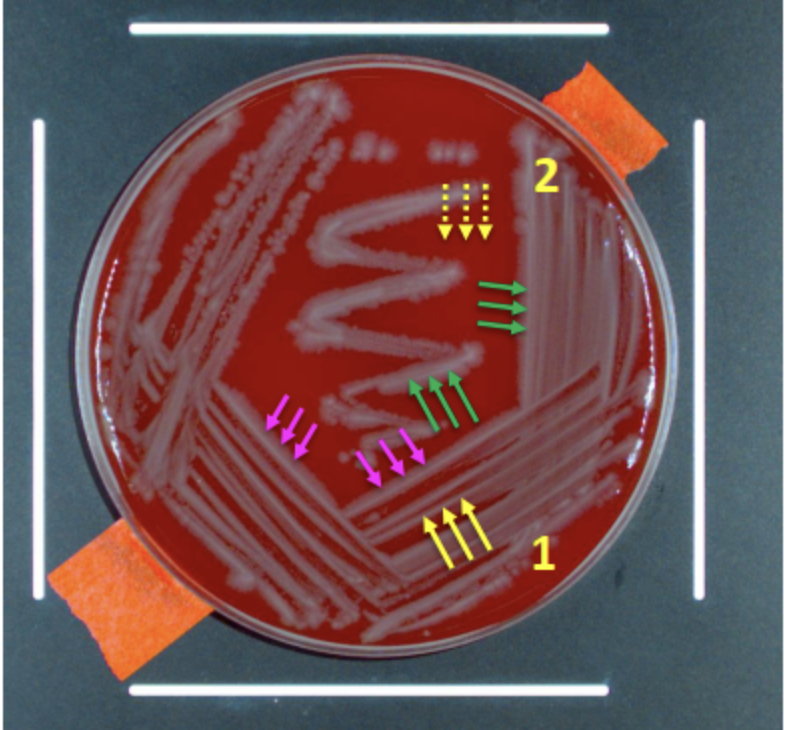
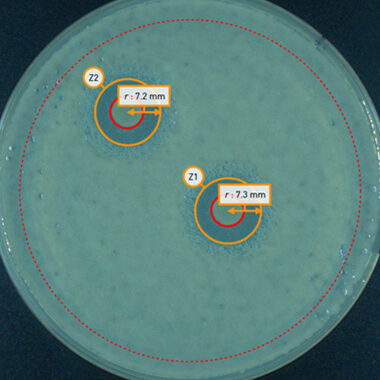
Automatic zone of inhibition detection and analysis with PIXL
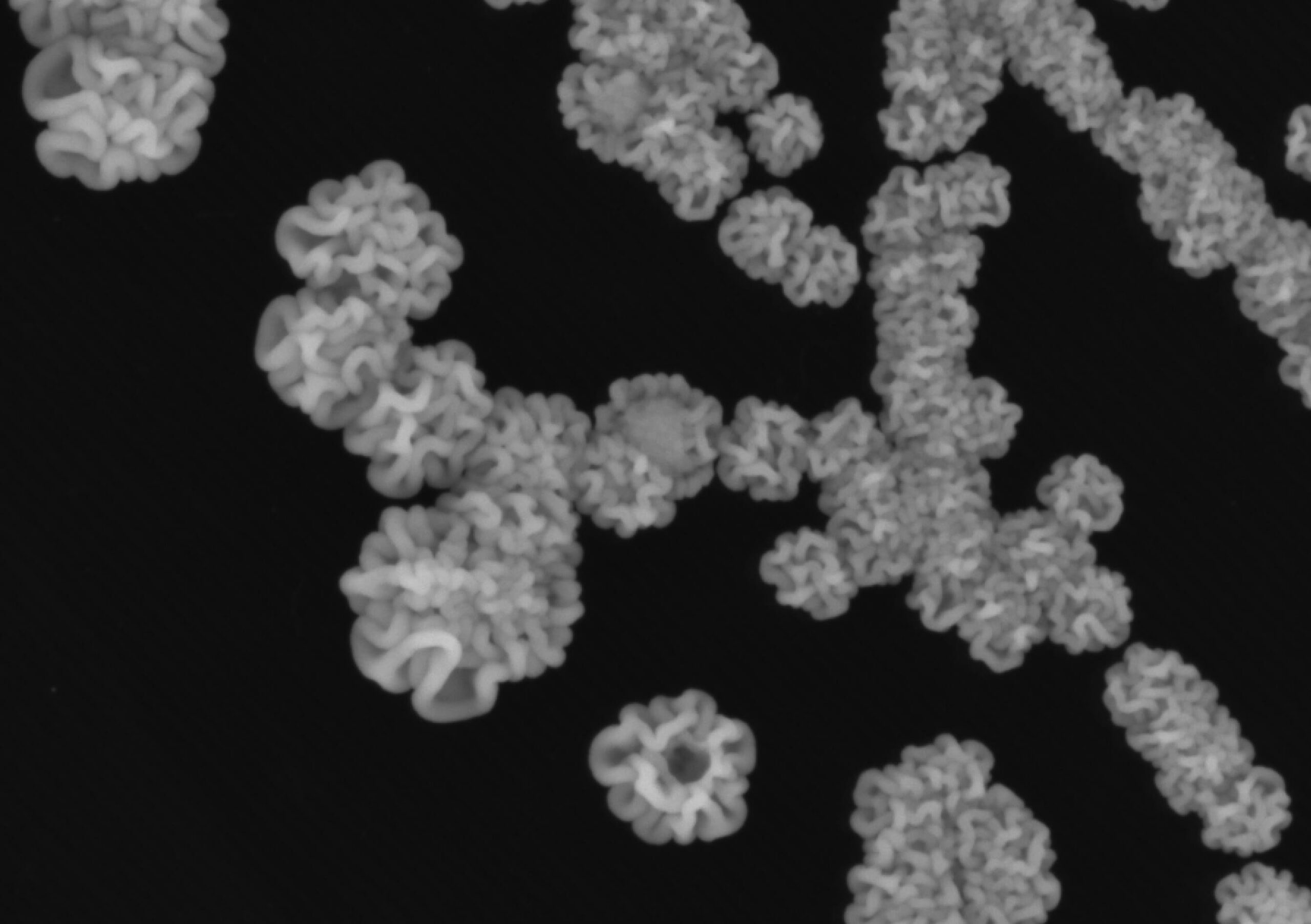
High-throughput bioprospecting: Automatic colony picking of non-model fungal and bacterial species
Six fascinating things you should know about cell cycle laureate Sir Paul Nurse
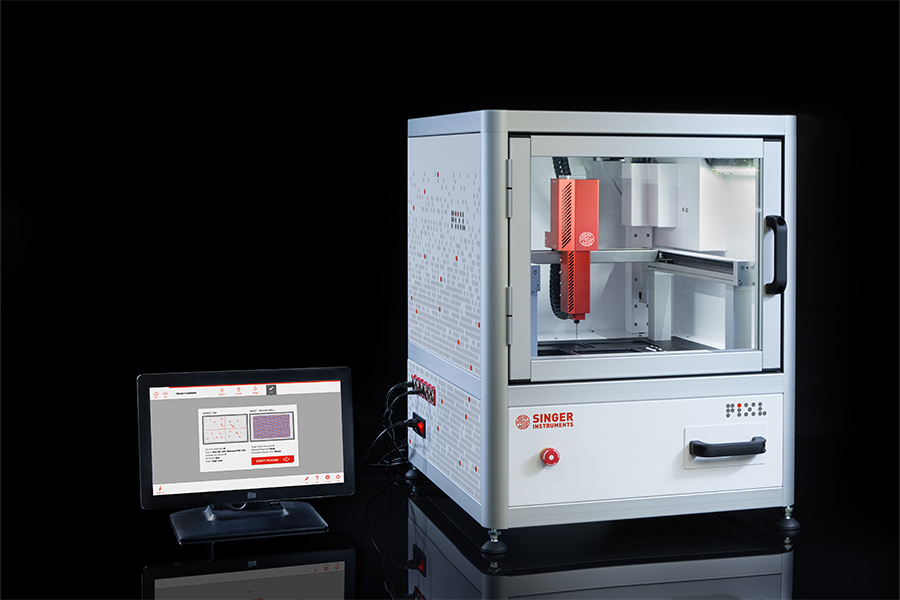
Elevate your Laboratory’s Colony Picking Automation
PIXL for Automated Colony Picking
High-throughput screening of green algae transformants
Designer chromosome synthesis with the help of PIXL
PIXL Pinning Pressure Report
PIXL Efficiency Report: Agar-Agar
What is High-Throughput Screening?
Book a 30-minute slot to discuss your workflow with one of our product experts, or ask us anything.
First Name
Last Name
Email*
Company/Institute*
How can we help?*
*I agree for my data to be used and stored as set out in the terms and conditions